Case of the Month – JULY 2026

Clinical Presentation
Q- A 25-year-old female presents with sudden-onset severe headache followed by progressive right-sided hemiparesis. CT head demonstrates subarachnoid hemorrhage, and digital subtraction angiography reveals a ruptured bilobed left ICA bifurcation aneurysm with severe vasospasm involving the supraclinoid ICA, ACA, and MCA territories.
What would you do next?
Abstract
Background: Management of intracranial aneurysms in the presence of cerebral vasospasm remains a formidable neurosurgical challenge. Vasospasm compromises cerebral perfusion, increases the risk of ischemia during temporary clipping, and complicates microsurgical dissection. Combined revascularization and aneurysm clipping may be considered in selected cases.
Observations: We report the case of a 25-year-old female who presented with a ruptured left internal carotid artery (ICA) bifurcation aneurysm associated with severe vasospasm and progressively worsening contralateral hemiparesis. She underwent a left pterional craniotomy with microsurgical clipping of the aneurysm along with an insurance superficial temporal artery to middle cerebral artery (STA–MCA) bypass. The aneurysm was successfully clipped, and bypass patency was confirmed intraoperatively. The postoperative course showed improvement in right hemiparesis and patient discharged in stable condition.
Lessons: STA–MCA bypass combined with aneurysm clipping is a viable strategy in cases with compromised cerebral perfusion due to vasospasm, ensuring both aneurysm exclusion and maintenance of adequate cerebral blood flow.
Introduction
Intracranial aneurysms arising at the internal carotid artery (ICA) bifurcation are technically demanding due to their deep location and proximity to critical neurovascular structures. Surgical treatment becomes considerably more challenging when associated with cerebral vasospasm following aneurysmal subarachnoid hemorrhage (aSAH). Microsurgical clipping remains a definitive treatment modality for such aneurysms. However, in cases where cerebral perfusion is compromised, adjunctive revascularization procedures such as superficial temporal artery to middle cerebral artery (STA–MCA) bypass may be necessary to maintain adequate cerebral blood flow and act as an insurance bypass to supplement impaired cerebral perfusion while aSAH-related cerebral vasospasm resolves after the acute insult over the ensuing weeks. Insurance and flow-alteration bypass techniques have been increasingly adopted in the management of complex intracranial aneurysms to reduce ischemic complications and preserve cerebral perfusion during microsurgical treatment. We present a case of ICA bifurcation aneurysm with vasospasm managed with combined clipping and bypass.
Case Presentation
A 25-year-old female presented to the emergency department with a history of sudden-onset severe headache of 5 days' duration, followed by development of right-sided hemiparesis over the preceding 24 hours, which was rapidly worsening to 2/5 (MRC grading). Non-contrast computed tomography (NCCT) (Fig. 1) of the head demonstrated subarachnoid hemorrhage (SAH) predominantly involving the anterior interhemispheric cistern, raising suspicion of a ruptured intracranial aneurysm. An emergent digital subtraction angiography (DSA) was subsequently performed, which revealed a bilobed aneurysm arising from the left internal carotid artery (ICA) bifurcation measuring approximately 5.5 × 7 mm with a 4 mm neck. In addition, severe vasospasm involving the supraclinoid ICA, anterior cerebral artery (ACA), and middle cerebral artery (MCA) was noted radiologically (Fig. 2, 3). Given the presence of a ruptured ICA bifurcation aneurysm associated with significant cerebral vasospasm and evolving neurological deficits, the patient was planned for urgent microsurgical clipping with concurrent cerebral revascularization.
Surgical Technique
Under general anaesthesia, the patient was positioned supine with the head extended and rotated to the right side around 30 degrees (Fig. 4, 5). A left frontotemporal curvilinear incision was made, and the parietal branch of the superficial temporal artery (STA) was harvested (approximately 8–9 cm) for bypass (Fig. 6). The STA remains the preferred donor vessel for low-flow cerebral revascularization because of its reliable caliber, accessibility, and favorable long-term patency.
A left pterional craniotomy was performed (Fig. 7). The sphenoid ridge was drilled to flatten the anterior skull base, and the dura was opened in a curvilinear fashion. Using a trans-sylvian approach, the arachnoid was widely dissected to expose the left ICA, proximal ACA, MCA, bilateral optic nerve, and ICA bifurcation. An aneurysm at the terminal ICA apex was identified along with vasospasm of the supraclinoid ICA, M1-MCA, and A1-ACA vessels (Fig. 8). Careful microsurgical dissection of the aneurysm neck was performed, preserving adjacent anterior cerebral artery (ACA) and middle cerebral artery (MCA) lenticulostriate perforators. Temporary proximal control was achieved using a temporary clip on the ICA (temporary clipping time: 2 minutes), followed by a permanent clip applied across the aneurysm neck (Fig. 9). Complete exclusion of the aneurysm with preservation of parent vessels was confirmed. Preservation of the parent ICA, ACA, and MCA branches was confirmed visually and using ICG angiography. No intraoperative rupture occurred, and blood clots in the subarachnoid space were evacuated.
Intraoperative indocyanine green video-angiography demonstrated delayed filling of the left MCA cortical vessels (Fig. 10), and the same findings were corroborated on intraoperative quantitative microdoppler readings (Hadeco, Japan). Subsequently, an insurance STA–MCA bypass was performed by anastomosing the harvested STA to an M4 cortical branch of the MCA (0.8 mm calibre) in an end-to-side fashion. Adequate flow through the bypass graft was confirmed intraoperatively using ICG video-angiography (Fig. 11) and microdoppler readings, which demonstrated augmented blood flow after bypass. Similar low-flow STA–MCA bypass techniques have been described as effective cerebral revascularization strategies for complex aneurysms requiring temporary or permanent flow alteration. Hemostasis was secured, and the wound was closed in layers after replacing the bone flap.
Postoperative Course
The patient was shifted to the intensive care unit in the immediate postoperative period. Neurological status showed gradual improvement, with motor power in the right upper and lower limbs improving from 2/5 preoperatively to 4/5 at the time of discharge on postoperative day 12. Serial transcranial Doppler studies were performed periodically and, interestingly, did not demonstrate elevated mean flow velocities in the left anterior cerebral artery (ACA) and middle cerebral artery (MCA), suggesting no progression of vasospasm observed preoperatively and intraoperatively. By the time of discharge, the patient was ambulatory without assistance (Fig. 12).
Discussion & Conclusion
The management of aneurysms in the presence of vasospasm is particularly challenging. Vasospasm reduces cerebral perfusion and increases the risk of ischemic injury during temporary clipping or vessel manipulation. The pterional approach with a trans-sylvian corridor provides excellent exposure of the ICA bifurcation while minimizing brain retraction. However, in the presence of vasospasm, even minimal vascular compromise can have significant neurological consequences. In this context, insurance STA–MCA bypass serves as a protective revascularization strategy, augmenting cerebral blood flow and reducing ischemic risk. This approach is particularly useful when there is significant vasospasm, prolonged temporary clipping is anticipated, or collateral circulation is inadequate. 65, 66] Previous studies have demonstrated that low-flow bypass procedures such as STA–MCA anastomosis can effectively maintain cortical perfusion in these settings and provide a valuable adjunct to definitive aneurysm exclusion while minimizing ischemic complications. The present case extends these concepts to a ruptured ICA bifurcation aneurysm complicated by severe diffuse vasospasm, where bypass was performed primarily to augment cerebral perfusion rather than facilitate parent vessel sacrifice.
Combined microsurgical clipping and STA–MCA bypass is an effective and safe strategy in selected cases of ICA bifurcation aneurysms associated with severe vasospasm. This approach ensures definitive aneurysm exclusion while maintaining adequate cerebral perfusion during the critical vasospastic period and may improve neurological outcomes in carefully selected patients.
Case Image Gallery
Click on any image to open the gallery view.
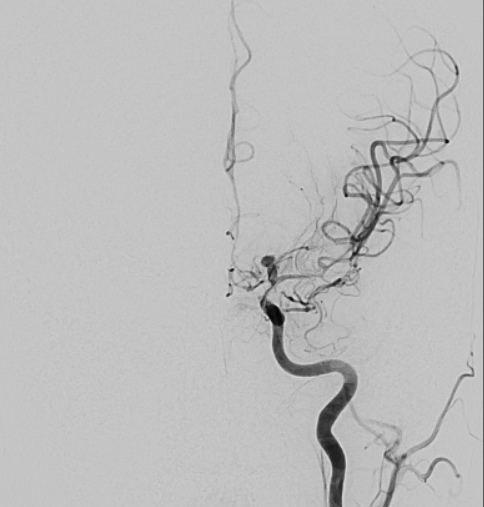
Fig 1. Non-contrast CT Head
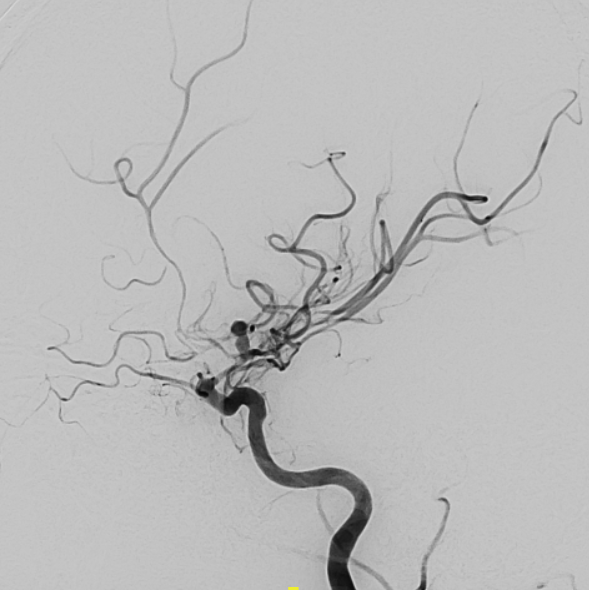
Fig 2. DSA (AP View)

Fig 3. DSA (Oblique View)

Fig 4. Patient Positioning
![Figure 5. Patient positioning for left pterional craniotomy- extended and rotated slightly to the opposite side]](assets/images/July Case Image/fig 6.png)
Fig 5. Patient Positioning (Alt)]
![Figure 6. Harvested graft- parietal branch of superficial temporal artery.]](assets/images/July Case Image/fig 7.png)
Fig 6. Harvested Graft (STA)]
![Figure 7. Left pterional craniotomy exposure.]](assets/images/July Case Image/fig 8.png)
Fig 7. Craniotomy Exposure]
![Figure 8. Intraoperative view of the ICA bifurcation aneurysm.]](assets/images/July Case Image/fig 9.png)
Fig 8. Intraoperative View]
![Figure 9. Final clip application at the aneurysm neck.]](assets/images/July Case Image/fig 10.png)
Fig 9. Final Clip Application]
![Figure 10. Intraoperative ICG angiography demonstrating absence of filling of aneurysm and delayed left MCA cortical filling.]](assets/images/July Case Image/fig 11.png)
Fig 10. Intraoperative ICG]
![Figure 11. STA–MCA bypass with confirmation of graft patency on ICG angiography.]](assets/images/July Case Image/fig 12.png)
Fig 11. STA-MCA Bypass Patency]
Want to join as a member